Author: Leonardo PilattiPhysiotherapist | Currently taking Master’s degree in Space Medicine Microgravity is a fascinating topic when it comes to the study of astronaut health. When humans are exposed to microgravity, the effects on their bodies can be quite significant. One of the first things to understand about microgravity is its effect on the musculoskeletal system. In the absence of gravity, astronauts experience a decrease in muscle mass and bone density. The lack of load-bearing activity in microgravity leads to muscle atrophy and bone loss. This can result in decreased strength and increased risk of fractures once astronauts return to Earth. Another area of concern in microgravity is cardiovascular health. On Earth, gravity helps to pump blood towards the lower extremities. In microgravity, this effect is greatly reduced, causing fluids and blood to shift towards the upper body. This can lead to a decrease in plasma volume. Astronauts often have to undergo intense exercise regimes during their space missions to counteract these effects. The immune system is also affected by microgravity. Studies have shown that the immune response of astronauts is suppressed during spaceflight. This can make them more vulnerable to infections and diseases. Researchers are still studying the exact mechanisms behind this phenomenon and are trying to find ways to boost the immune system during space missions. Microgravity also has an impact on the astronaut's vision. Some astronauts have reported changes in their vision, such as an increase in visual blurring and other visual disturbances. This condition, known as spaceflight-associated neuro-ocular syndrome (SANS), is still being studied to understand its underlying causes and potential long-term effects. In addition to physical health, microgravity can also impact an astronaut's mental well-being. The unique environment of space, with its isolation, confinement, and lack of natural daylight, can lead to psychological challenges such as mood swings, sleep disturbances, and increased stress. NASA and other space agencies provide mental health support and psychological training to help astronauts cope with these challenges. 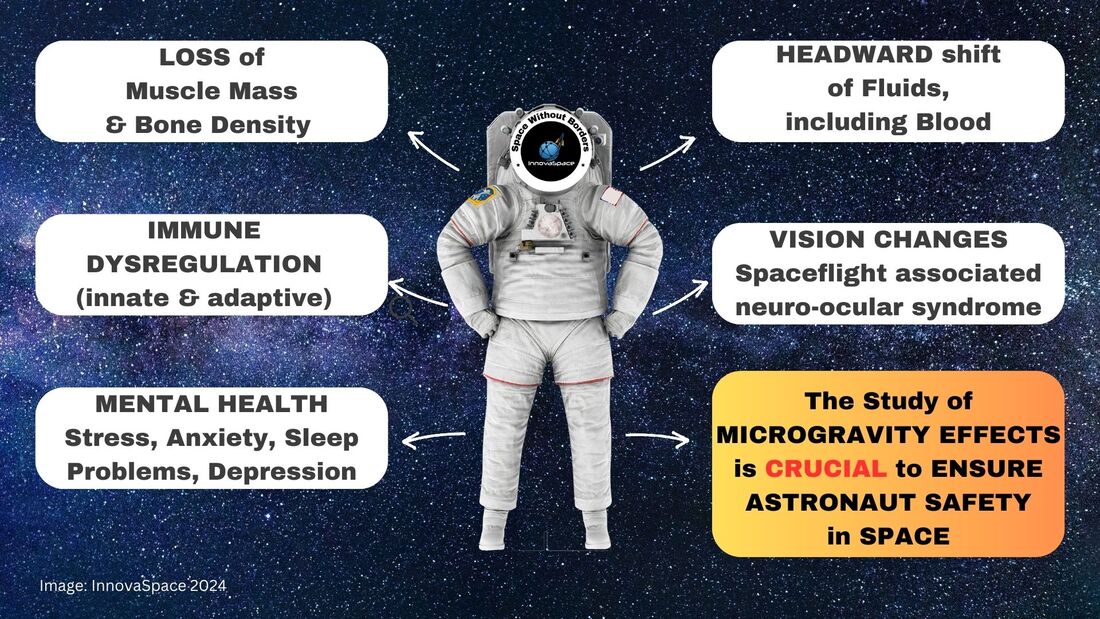 To mitigate the negative effects of microgravity on astronaut health, space agencies invest in various countermeasures. These include exercise programs, special diets, and even medications. Additionally, researchers are constantly studying new technologies and strategies to protect and enhance astronaut health during long-duration space missions.
In conclusion, microgravity has significant effects on astronaut health, impacting various systems in the body. The study of these effects is crucial to ensure the well-being and safety of astronauts during space missions. By understanding and addressing these challenges, we can continue to push the boundaries of space exploration while also safeguarding the health of those who venture into the final frontier. Author: Tobias LeachMedical Student, University of Bristol | iBSc Physiology at King’s College London  The first edition of the InnovaSpace Journal Club was dedicated to a prospective cohort study on jugular venous flow in astronauts aboard the ISS. From this study, the issue of jugular vein thrombus formation arose, which led to some fascinating discussion on how we could possibly manage and mitigate this novel risk to astronaut health. Therefore, I thought it appropriate to use the second edition of the InnovaSpace journal club to cover the issue of bleeding in space. Major Haemorrhage in space – How can it arise? How can it be managed? Should we worry about it?  PAPER PRESENTED & DISCUSSED:  We used a 2019 literature review which evaluated different haemostatic techniques in remote environments and proposed a major haemorrhage protocol for a Mars mission.
The article itself stressed that while the estimated risk for major haemorrhage on a Mars mission was not very high, there were still many possible causes for a big bleed such as trauma and high dose radiation. Additionally, the changes to circulatory physiology observed in microgravity may mean astronauts are less able to cope with even small amounts of blood loss. While the literature search itself left a lot to be desired as only 3 of the 27 papers were randomised controlled trials (RCTs), the results were interesting. Author: Lucas RehnbergNHS Doctor - Anaesthetics & Intensive Care | MSc Space Physiology & Health   My name is Lucas, I am a doctor in the UK working in anaesthetics (or Anaesthesiology for any American readers) and intensive care medicine. I have had an interest in space medicine for over 10 years now, inspired by none other than Prof Thais Russomano who has mentored me over the years and still does. My Master’s dissertation (back in 2009) focused on CPR (cardiopulmonary resuscitation) methods in microgravity, with my continued research interest surrounding critical care in space. I am careful to say that I am a doctor with an interest in space medicine and physiology, as opposed to a ‘Space Doctor’ – as there are many individuals out there who have committed many more years than I have to this field and are vastly more experienced than I am! A club I aspire to join one day. The idea of this blog, or series of blogs, is to look at some of the latest research in space physiology and space medicine, then consider how this will play out clinically. With a particular focus on critical care and potentially worst-case scenarios when in space (or microgravity environment). Something all doctors will have done in their careers; we are equipped with the skills to critically appraise papers and then ask if they are clinically relevant, or how will it change current practice. Over the last 60 (ish) years of human space flight, there is lots of evidence to show that there are many risks when the human body has prolonged exposure to microgravity, which can affect most body systems – eyes, brain, neuro-vestibular, psychological, heart, muscle, bone, kidneys, immune system, vasculature, clotting and even some that we haven’t fully figured out yet. But then what needs to be done is to tease out how clinically relevant are these from the research, how could that potentially play out if you were the doctor in space, then how to mitigate that risk and potentially treat it.  Author: Tobias Leach3rd Year Medical Student | University of Bristol | Passionate about space!  Space provides boundless opportunities for human existence and innumerable threats to human health. The question is, are we yet prepared to deal with a catastrophic event, such as a cardiac arrest in space? Abstract
Introduction To gain an understanding of the current state of CPR in microgravity with a focus on chest compressions in the event of a sudden cardiac arrest onboard. Methods An Ovid Medline search was conducted: 17 articles were found; 12 were excluded; six additional articles were found in the references of the remaining five articles, bringing the total number of articles included to 11. These were then critically analysed. Results No CPR method currently reaches the European Resuscitation Council (ERC) guidelines. The Handstand (HS) method appears to be the strongest. Evetts-Russomano (ER) is the second strongest method. Automatic chest compression device (ACCD) performed consistently well. Conclusion CPR appears to be far more difficult in microgravity. Inconsistencies in research methodology do not help. The ER method should be used as a first contact method and the HS method should be used once the casualty is restrained. An ACCD should be considered as part of the medical equipment. Further research is needed, directly comparing all positions under the same conditions. Author: Paul Zilberman MDAnaesthesiologist, Israel MOTTO: I was born in 1960. As a child I was thrilled to witness the first man in space, as per stories, in those years a direct TV transmission was still a dream. And even if it had been possible, I was one year of age, so… But later on, I was able to see the launch of the Apollo missions and the common US-Soviet programs Soyuz- Apollo. As many other terrestrials I was thrilled to watch, both from distance and close up, those “white pencils” with the painting of “The United States of America” climbing faster and faster, leaving behind a huge ball of fire… Then the first carrying rocket segment detaching and falling back to Earth… I was amazed seeing how only after a short time those “people out there” were floating and smiling, waving their hands and telling us everything is ok. I was reading about the many experiments that were carried out during the flights, I was even able to look now and then at the flight path, little understanding what were the sinusoidal lines appearing on the huge Command Center screen, where so many people were sitting in front of the computers with the microphones and earpieces connected. I didn’t understand then, exactly, why so many people were dealing with so few in space.
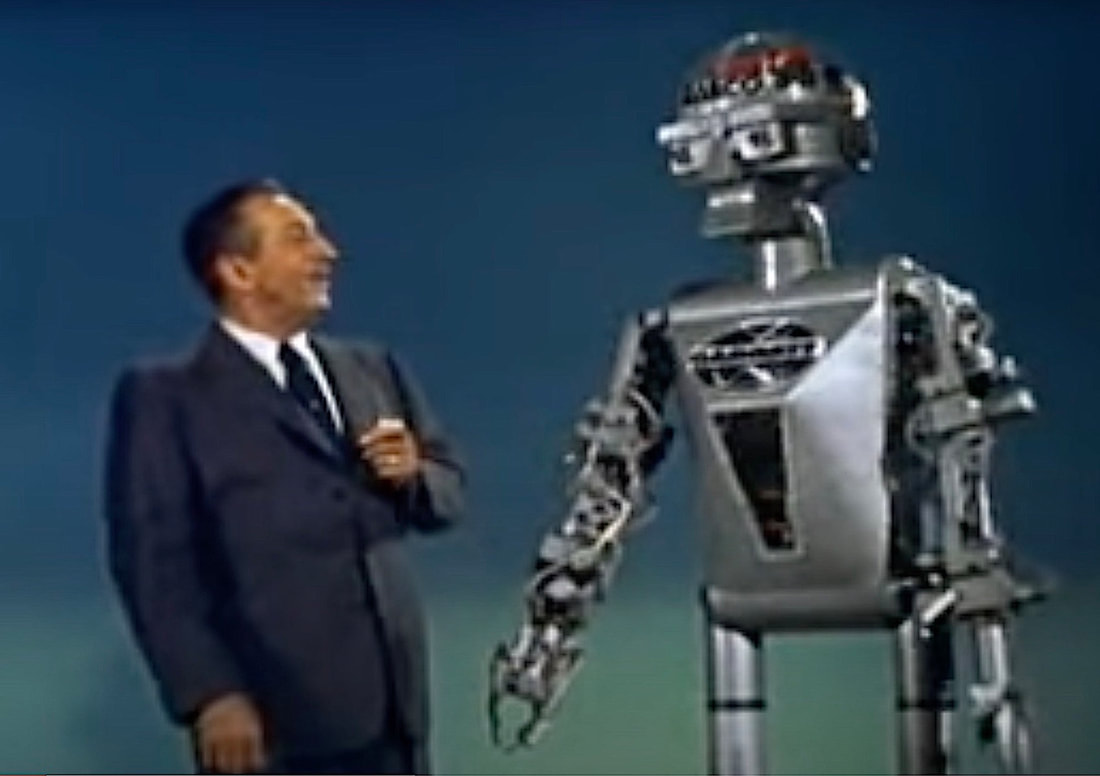
Well, time went on, Skylab appeared, then the ISS, the shuttles…wow…all in a lifetime. As time went on and understanding grew, on top of my medical school and, later on, anaesthesia residency, other questions arose: how do the astronauts eat, drink, wash, use the toilets? And many other daily mundane things we take for granted down here. Author: Rohan KrishnanUndergraduate, Bachelor of Science - Statistics & Healthcare Management | The Wharton School, University of Pennsylvania In 1955, Walt Disney’s “Mars and Beyond” pondered human survival in extraterrestrial environments. The narrator envisions the colonisation of Mars as a feasible reality: a future where cities are encased in pressurised domes on the Red Planet to combat overpopulation and the depletion of natural resources on Earth.
Today, NASA’s Artemis Mission plans to return astronauts to the moon by 2025, this time with an eye toward lunar colonization and human exploration of Mars. The boundaries that once constrained human space exploration are shattering, as technological advancements and ambitious government space programs bring plans for travel to Mars closer to reality. Beyond government space agencies, private companies like Blue Origin and SpaceX are innovating to create faster, more efficient aircraft and bring space travel to the masses through commercial flights. As astronauts inch toward deep space missions, understanding the general health risks of long-distance space travel, as well as the varied conditions between environments, is crucial. Missions to the International Space Station (ISS) and in low Earth orbit (LEO) have uncovered a variety of consequences for astronaut health, including bone loss, muscle atrophy, and a weakened immune system, amongst others. Radiation, microgravity, the distance from Earth, isolation, and the hostile environment inside spacecraft are the root causes behind the health issues that astronauts experience in space. Space exploration is vital for advancing life on Earth. Future missions across our solar system can help us understand the effects of microgravity and radiation on biological systems, locate valuable natural resources, and even combat overpopulation by exploring space colonisation. Given this need, ensuring the health of humans in space is the bedrock for further discovery. 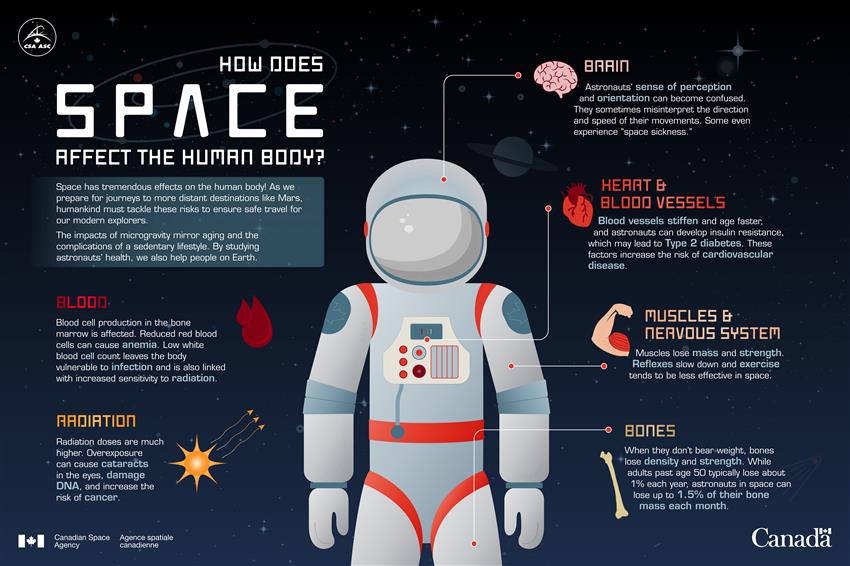 How space affects the human body – Infographic. (Credit: Canadian Space Agency) In this blog, I will describe the significant health challenges associated with with spending time in LEO and on long-distance spaceflight to the Moon and Mars. I have narrowed the focus to the following branches of medicine, to outline and contrast the particular health issues between LEO and long-distance spaceflight: cardiology, ophthalmology, and neurology. Many of the health concerns associated with time spent in LEO persist during long-distance space travel, but there are also challenges specific to the Moon and Mars stemming from their unique environmental characteristics, such as the presence of regolith and varying radiation levels. Understanding these general and environment-specific health concerns will inform planning as we venture deeper into space. The vast majority of human spaceflight has occurred within low Earth orbit (LEO), with the notable exception of the Apollo program’s lunar missions. All manned space stations, including the ISS, are in LEO. As a result, for more than two decades, countless experiments have been conducted on the ISS to understand how astronauts’ health is impacted in LEO.

CardiologyResearchers studying the health of astronauts aboard the ISS have uncovered that long-term travel in LEO has notable effects on astronauts’ cardiovascular health. According to Dr. Thais Russomano, a leading expert on space medicine, the absence of Earth’s gravitational force in space causes bodily fluids and blood to shift from the legs and lower abdomen toward the upper torso and head. This phenomenon - referred to as ‘puffy-face and bird-legs syndrome’ - causes swelling in the face and head while reducing astronauts’ circulating blood volume and heart size. As less blood is pumped by the heart in microgravity, astronauts endure muscle loss in the heart, placing them at risk for cardiovascular deconditioning and cardiac myocyte atrophy.
Radiation is another significant concern impacting astronauts’ cardiovascular health. Aboard the ISS, radiation from galactic cosmic rays, solar cosmic rays, and particles from the Van Allen radiation belts are of primary concern. Astronauts are exposed to roughly 40-times more millisieverts of radiation compared to people on Earth. Exposure to space radiation over long-term missions increases astronauts’ risk for cancer and cardiovascular diseases, although effective shielding and radiation shelters aboard spacecraft have helped mitigate those risks. Cardiovascular issues resulting from microgravity and radiation exposure over long periods aboard the ISS can follow astronauts well after returning to Earth. Some studies have determined that astronauts’ arterial blood pressure decreased throughout space missions due to the loss in circulating blood volume, although there could be many causes behind this change. Similarly, the reduction in circulating blood volume can cause orthostatic intolerance - the inability to stand due to lightheadedness or fainting - once astronauts return to Earth. Although radiation exposure and microgravity cause cardiovascular problems in space, studies on astronaut mortality have concluded that astronauts are at a lower risk of death from cardiovascular diseases relative to the general population on Earth. OphthalmologyThe effects of bodily fluid shifting in microgravity extend beyond ‘puffy-face and bird-legs syndrome’, with consequences for the eyes. Following a six-month mission to the ISS in 2005, astronaut John Phillips’s perfect vision was found to have deteriorated due to spaceflight-associated neuro-ocular syndrome (SANS). SANS is formerly known as visual impairment and intracranial pressure (VIIP) syndrome, although the name was updated to reflect the uncertainty over whether increased intracranial pressure is the sole cause of the condition. One explanation is that SANS is caused by cerebrospinal fluid shifting toward the head, increasing intracranial pressure, particularly at eye level. The pressure causes the back of the eye to flatten, resulting in a hyperopic shift and blurred vision.
According to a report from the British Journal of Anaesthesia, a questionnaire of 300 astronauts found that 28% of short-duration mission astronauts and 60% of long-duration mission astronauts experienced degradation of visual acuity. A study of seven long-duration mission ISS astronauts and nine short-duration mission space shuttle astronauts found that the long-duration astronauts had significantly greater post-flight flattening when compared with the short-duration astronauts. Given the increased severity of SANS on long-duration missions, understanding causes and possible treatments are vital for exploration in and beyond LEO. NeurologyMicrogravity has notable effects on the nervous system, particularly due to the redistribution of bodily fluids in space. Neuroimaging scans show that astronauts’ brains have increased ventricular volumes following long-distance spaceflight. As fluids shift toward the upper torso and head during long-term exposure to microgravity, the volume of cerebrospinal fluid collected in the brain’s ventricles increases, resulting in ventricular expansion. Ventricular expansion could be a possible cause of SANS and may be linked to premature ageing of the brain. One study found that astronauts who spent 12 months in space displayed larger changes in ventricular volume than astronauts who spent 6 months in space, suggesting important implications for long-duration space missions. The microgravity-induced fluid shift is also associated with alterations to white matter in astronauts’ brains. A study from the journal Science Advances reports that cosmonauts displayed increased white matter in the cerebellum following long-duration spaceflight, with white matter volume returning to roughly pre-flight levels seven months after spaceflight. The cerebellum handles fine motor control, postural balance, and oculomotor control, and white matter changes associated with spaceflight may offer evidence for motor system neuroplasticity. Various studies are employing different techniques to evaluate white matter changes due to spaceflight, which could affect other neurological functions including visual and sensory processing. The health issues associated with LEO are also relevant for long-distance space travel. However, there are also environment-specific challenges unique to the Moon and Mars - such as high levels of space radiation and varying magnitudes of microgravity - that will be of primary concern to astronauts. Various studies simulate deep space environments to predict the effects of long-distance spaceflight on human health, informing mitigation strategies to keep astronauts safe.
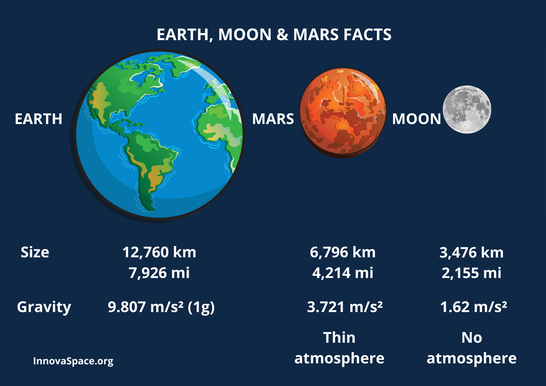
CardiologyIn deep space, the microgravity environment induces similar cardiovascular effects to what astronauts experience in LEO. Blood and bodily fluids shift toward the upper torso and head resulting in ‘puffy-face and bird-legs syndrome’, while the decreased cardiac workload can lead to cardiovascular deconditioning. However, relative to the gravitational force in LEO of approximately 0.95g, the Moon’s gravitational force is 0.16g while Mars’ gravitational force is 0.36g. It is unclear whether varied microgravity conditions will produce additional cardiovascular effects beyond those studied in LEO, however, fluid shifts and cardiovascular deconditioning remain significant concerns.
Radiation-induced cardiovascular disease is another major challenge with traveling to the Moon and Mars. Compared to missions in LEO, the space radiation environment beyond LEO exposes astronauts to higher dose rates of HZE particles, the high-energy heavy ions of galactic cosmic rays. HZE particles are highly penetrating and can cause secondary radiation when interacting with shielding in spacecraft or spacesuits. According to the journal Frontiers in Cardiovascular Medicine, high doses of HZE particles over long-term deep space missions can lead to myocardial remodelling and fibrosis, potentially resulting in heart failure. While current shielding technology may protect astronauts in LEO, the power of HZE radiation makes more advanced shielding essential to protect astronauts in deep space. OphthalmologyConsidering the microgravity-induced fluid shifts that astronauts experience in deep space, SANS remains a primary concern for missions to the Moon and Mars. SANS is typically studied on long-duration missions, although astronauts have reported blurred vision after only two weeks aboard the ISS. A mission to Mars would take up to 20 months and would require astronauts to encounter multiple gravity fields. The long duration and complex gravity shifts associated with deep space missions could cause more challenging SANS-related ocular issues compared to those faced by astronauts in LEO. The concerns surrounding radiation beyond LEO extend to ocular health. Galactic cosmic radiation has been linked to the development of phosphenes and cataracts, while studies show that repetitive spaceflights and high-radiation-dose exposure increase the prevalence of both conditions among astronauts. Considering the high volume of HZE radiation that deep space astronauts will be exposed to, the development of phosphenes and cataracts is of major concern for their ocular health.
NeurologyPrevious studies have sought to evaluate the effects of space radiation on the human brain by delivering radiation doses to rodents over a few minutes. However, on missions to the Moon and Mars, powerful radiation will be gradually delivered to astronauts for the duration of the trip, ranging from weeks to years. A 2019 study from the journal eNeuro aims to more accurately simulate long-duration exposure by delivering low-level neutron radiation to mice for six months and evaluating the neurological implications. The study finds that exposure to cosmic rays impairs the brain function of the mice, affecting learning, memory, and mood. Lab tests reveal that following the neutron radiation, neurons are less responsive in the hippocampus - an area critical for the formation of memories and spatial navigation - and the medial prefrontal cortex - an area responsible for accessing preexisting memories, decision-making, and processing social information. Follow-up evaluations of the irradiated mice determine that neural circuitry damage may last for up to one year. Some researchers dispute the study’s approach, claiming that neutron radiation used in the experiment is not a viable surrogate for the galactic cosmic radiation that astronauts would encounter during deep space missions. Still, the eNeuro study offers a novel analogue to the gradual doses of powerful space radiation that astronauts would face on missions to the Moon and Mars, further emphasising the importance of effective shielding from cosmic rays. Researchers are also studying how microglia - the immune cells of the central nervous system - can be manipulated to prevent the development of cognitive deficits due to galactic cosmic ray exposure, a promising step toward protecting astronauts on deep space missions.  ConclusionMotivated government leaders and entrepreneurs alike have expressed their commitment to bringing the human race beyond low Earth orbit. As breakthroughs in deep space research and aerospace technology bring this goal closer to realisation, concomitant advancements in space medicine must be made to safeguard astronauts’ health as they travel to and thrive in extraterrestrial environments. Before we can walk on Mars, our first step must be understanding and mitigating the health challenges that await us deeper into the final frontier. Author: The InnovaSpace TeamSpace Without Borders! InnovaSpace CEO Thais Russomano recently contributed an article to the magazine - Asian Hospital & Healthcare Management - examining the challenges humankind faces if we are to spend more time in space. It gives a good overview of the topic without being too technical and is open access, so we thought you might like to take a look!  The article features on pages 6-9 of the magazine and you can download the magazine free by following this LINK
Author: Hamzah RahmanYear 3 student - Guy's, King's and St Thomas' School of Medicine & Space Enthusiast!  de Havilland Comet aircraft de Havilland Comet aircraft The General Practitioner (GP) medical professional has undoubtedly played a major role in providing a plethora of care packages and programmes for individuals seeking to travel; from immunisations and vaccinations to advice and even guidance for mothers in the late gestational stage. The advent of jet flight allowed the masses to venture to destinations that only aristocracy could once afford, which in turn generated a greater need for primary healthcare management. The GP is therefore the point of access to these healthcare packages and consequently plays a pivotal role in enabling tourists to travel safely. This responsibility is deeply intertwined with the historic increase in accessibility to affordable flight. The first British commercial jetliner was the de Havilland Comet in 1949. This aircraft enabled more people to travel further, as well as reducing the price of tickets substantially. The GP during this age would have played an important role in ensuring that passengers were fit to fly, by managing their pre-flight healthcare requirements.  Boeing 747-121 | Image credit: Aldo Bidini Boeing 747-121 | Image credit: Aldo Bidini The Boeing 707 soon joined the aviation world in 1957 and dramatically changed the way we travelled; it opened flight corridors that were once untenable, and consequently, accessed a greater consumer market - the working classes. In 1969, Boeing unveiled the revolutionary 747, coined the “Jumbo Jet” due to its sheer size, which resulted in greater passenger capacity and far more affordable tickets. With such quantum leaps forward in jet aviation, by the mid-70s the British GP was providing care and advice to thousands of travellers from all walks of life, different backgrounds and with all manner of pre-existing health conditions. The workload of the GP thus became much more diverse and they gained great responsibility in permitting the public to exercise their freedom to travel safely. Just as jet flight was once an exclusive mode of transport for those from higher socio-economic backgrounds, spaceflight has now emerged onto the world market with exclusive and expensive tickets to fly. Undoubtedly, spaceflight will become more affordable in the coming years and decades, and as such will inevitably require a more established initial healthcare access point for travellers- a service that GPs could provide. As space tourism flights become more accessible through lower prices and increased provision, the remit of travel healthcare provided by general practice could evolve in the near future to encompass spaceflight health clearance.
 Cardiopulmonary resuscitation (CPR) is a well-established part of basic life support (BLS), having saved countless lives since its first development in the 1960s. External chest compressions (ECCs), which form the main part of BLS, must be carried out until Advanced Life Support can begin. It is essential that ECCs are performed to the correct depth and frequency to guarantee effectiveness. The absence of gravity during spaceflight means that performing ECCs is more challenging. The likelihood of a dangerous cardiac event occurring during a space mission is remote, however, the possibility does exist. Nowadays, the selection process for space missions considers individuals at ages and with health standards that would have prohibited their selection in the past. With increased age, less stringent health requirements, longer duration missions and increased physical labour, due to a rise in orbital extravehicular activity, the risk of an acute life-threatening condition occurring in space has become of greater concern. The advent of space tourism may even enhance this possibility, with its popularity set to rise over the coming years as private companies test their new technology. Therefore, space scientists and physicians will have a greater responsibility to ensure space travellers, whether professional astronauts or space tourists, are adequately trained and familiarised with extraterrestrial BLS and CPR methods. Recently, work has been undertaken to develop methods of basic and advanced life support in microgravity and hypogravity, and several CPR techniques have been developed and tested. This blog presents one of these, the Evetts-Russomano MicroG CPR Method. Evetts-Russomano MicroG CPR Method In the Evetts-Russomano (ER) method, the rescuer can respond immediately, as it requires no additional CPR equipment/medication or the use of a restraint system. To assume the position, the rescuer places their left leg over the right shoulder of the patient and their right leg around the patient’s torso, allowing their ankles to be crossed approximately in the centre of the patient’s back; this is to provide stability and a solid platform against which to deliver force, without the patient being pushed away. From this position, chest compressions can be performed while still retaining easy access to perform ventilation. When adopting the ER CPR method, the rescuer must be situated in a manner that also allows sufficient space on the patient’s chest for the correct positioning of their hands to deliver the chest compressions. Extraterrestrial CPR simulation The main difference between extraterrestrial and terrestrial CPR is the strength of the gravitational field. In microgravity, patient and rescuer are both essentially weightless. When thinking about the technique of terrestrial CPR, with the rescuer accelerating their chest and upper body to generate a force to compress the patient’s chest, it is obvious that this cannot work in microgravity without significant aids. To this end, the ER CPR method has been developed using a ground-based microG simulation, during parabolic flights, and subsequently tested under-water! Video credits: Ground-based MicroG Simulation (land) = Space Researcher Lucas Rehnberg, MD (MicroG Center PUCRS, Brazil) Parabolic Flight MicroG Simulation (air)= Researchers = Thais Russomano, Simon Evetts, Lisa Evetts & João Castro (ESA 29th Parabolic Flight Campaign, Bordeaux, France) Underwater MicroG Simulation (water) = Sea King Dive Center, Chengdu, China - Instructor Gang Wei; Chinese Space First Responder & Space Researcher/Instructor Chris Yuan A project of InnovaSpace, PECA and Guangxi Diving Paradise Club, China Free Resource: Extraterrestrial CPR and Its Applications in Terrestrial Medicine
Authors: Thais Russomano, Lucas Rehnberg In book: Resuscitation Aspects, Ed: Theodoros Aslanidis Publisher: IntechOpen 2017 See Download Link at https://www.innovaspace.org/chapters.html Luis E. Luque Álvarez, M.Mus.Ed.Violin Teacher, Kittenberger Kálmán Primary & Arts School, Nagymaros, Hungary. Member of ELGRA Across centuries playing and listening to music has been an important human psycho-physiological communication path with or without lyrics. It is clear that in space sciences music has intervened in the life of most scientists as a motivational and alternative health resource. Pythagoras of Samos studied the physiological effect of certain scales and melodies on the human body, he believed each different modal scale would induce a different mood state to the listener or player. Several astronomers like the Galilei family, and William and Caroline Herschel, among others, were strongly connected to music, indeed they were exceptional musicians themselves.
And it was during the Apollo 9 mission when Rusty Schweickart carried a Sony Tape recorder, strictly for the purpose of providing a musical environment for the astronauts. Since then, astronauts have often highlighted the importance of music for their mission performance and have taken their music with them, indeed a tradition of wake-up calls from Mission Control has long been established to begin the astronauts’ days. These anecdotes indicate how strong is the importance of music, at least psychologically, perhaps physiologically too, for astronauts under the stress and pressures caused by the confinement of a spaceflight mission. Music for Space ProjectAs a music student in 2016 I became curious about the idea of experimenting with the effect of listening to and playing music in space. At that time, I didn’t find much scientific literature about the effects of music in microgravity, hypogravity or hypergravity. Music has been highlighted only as a leisure practice and for psychological support, though I believe it provides much more than that. In 2018, I was lucky enough to have the support of the ESA Education Office, DLR, European Astronaut Centre and the European Low Gravity Research Association, teaming up with some French and Hungarian students to perform a first experiment using personalized music intervention as a psycho-physiological countermeasure under exposure to hypergravity in a Short Arm Human Centrifuge. During the ESA Spin Your Thesis Human Edition programme, our student team, along with two others (SpinKings and Spin Doctors), were able to perform some very interesting research in different space physiology fields. Our research involved 10 male participants, divided equally into two groups of 5, and spinning them in the centrifuge at 1Gz and 1.5Gz of hypergravity, with one group listening to a different style of music per spinning protocol, while the other group were spun without music. We recorded many different variables, including sociocultural background, psychological mood states, muscle tone, and galvanic skin response, among others.
Preliminary results have shown there is a clear tendency in the effect of music to decrease the tension, anxiety levels compared with the control group without music, and there was a certain stabilisation of stress muscles, which previous centrifuge studies have shown to be affected in a different way. Currently, the data is being re-analysed with the cooperation of scientists at ESA aiming to publish the complete data results. Since the Spin Your Thesis Human Edition campaign, the audio device with stereo signal installed specifically for the music experiment still remains attached to the short arm human centrifuge, where nowadays ESA astronauts and study participants can enjoy their favourite music playlist on the centrifuge. This experiment was the initial phase of the Music For Space project, which aims to continue the research with music as a psycho-physiological countermeasure to improve astronaut’s health with alternative medicine methods and perhaps one day for Earth citizens as well. We have in music history thousands of music styles, genres, instrumentations, and performance versions. To determine their specific benefits or disadvantages, we would need to perform more terrestrial tests, such as using a human centrifuge, parabolic flights, and analog simulations. In addition to music listening, I aim to measure in space how the playing of musical instruments could support brain, muscles, and bone health. Further studies could lead us to obtain enough data to approach an adequate and systematic music therapy method for spaceflight crews. I encourage all students and young researchers from fields that seem to be far from space sciences to feel curious, to pursue your dreams and to try the student experiments offered by the ESA Education Office. These are an unforgettable life experience and a wonderful opportunity for students to contribute to space-related research.
 |
Welcometo the InnovaSpace Knowledge Station Categories
All
|









 RSS Feed
RSS Feed